Can You Have ADHD Without Hyperactivity? 3 Overlooked Truths
TLDR: The diagnostic term for this condition is ADHD-PI, which stands for predominantly inattentive presentation. The older label ADD was officially retired in 1994, but it still circulates in everyday conversation. To find real answers, we have to look past the old stereotypes and understand how the inattentive brain actually processes the world.
At 24, I sat in front of a screen and poured my heart out to a stranger I had never met. It was my first telehealth session. After listening to me for a few minutes, she said confidently, “You sound like you may have adult ADHD.” I laughed out loud.
Her comment made me wonder: Can you have ADHD without hyperactivity? I was completely exhausted most of the time, overwhelmed, and scatterbrained, but I was not hyperactive. I definitely was not bouncing off the walls.
That reaction is exactly why so many adults with ADHD go years without a proper diagnosis. The condition they have is real, medically diagnosable, and officially classified under the American Psychiatric Association DSM-5, but it does not look the way the public expects it to look.
Women with ADHD are diagnosed an average of five years later than men, largely because inattentive symptoms appear quiet and internal. The cost of this late diagnosis is not abstract: it leads to mental health treatments that never address the root issue, overlapping conditions like chronic anxiety, and a growing internal conviction that the problem is a personal failure rather than a neurological reality.
By the end of this post, you will understand exactly what inattentive ADHD is, why it goes undiagnosed more often than not, and what the first steps toward a clinical evaluation look like.
Can You Have ADHD Without Hyperactivity?
ADHD without hyperactivity is the predominantly inattentive presentation of ADHD, a neurodevelopmental condition defined by chronic difficulty sustaining attention, organizing tasks, and following through. It occurs without prominent physical restlessness or behavioral impulsivity.
The historical name Attention Deficit Disorder (ADD) officially changed to Attention-Deficit/Hyperactivity Disorder (ADHD-PI), predominantly inattentive presentation, with the release of the DSM-IV in 1994.
That major clinical shift recognized ADHD as a single disorder with three distinct symptom clusters instead of two completely separate conditions. Doctors, teachers, and older clinical resources kept using the acronym ADD long after the switch, which is why the outdated name persists today.
A formal diagnosis carries the same clinical threshold as any other presentation: an adult must meet five or more inattention symptoms under the DSM-5 guidelines. These symptoms must be present across multiple settings, persist for at least six months, and have a clear onset before age 12.
The presence of the word hyperactivity in the full medical name of the disorder does not mean every person with ADHD experiences it.
Among adults who have received a diagnosis, 31% present with the inattentive-only subtype, 62% present with the combined subtype, and the hyperactive-only presentation accounts for just 7%.
These figures, documented in a landmark study on Adult ADHD Subtype Presenting Symptoms published in The Journal of Clinical Psychiatry, prove that in the adult population, the public image of ADHD: the fidgeting, the interrupting, the person who cannot sit still, describes a small minority of cases, not the vast majority.
How ADHD Without Hyperactivity Works in Practice
The Attention System Fails Differently
In inattentive ADHD, the core dysfunction is not that the brain refuses to pay attention. The reality is that the brain cannot reliably regulate what should receive attention.
The executive function networks responsible for initiating tasks, filtering out background noise, holding information in working memory, and shifting focus at the right moment are unstable, not absent. My brain’s experience with inattentive ADHD is best described as a scrambled egg, mid-scramble, most of the time.
Clinical models popularized by Dr. Russell Barkley on ADHD Executive Dysfunction argue that ADHD is fundamentally a disorder of executive functioning and self-regulation, not a simple attention deficit.
For the inattentive presentation, this manifests as a task that feels physically impossible to start despite high real-world stakes; a conversation where the first sentence lands clearly, but the rest dissolves into background noise; or a checklist completed six times in your head but zero times on paper.
Hyperactivity Can Be Internal
While many people with inattentive ADHD show little if any physical hyperactivity, it is a near-universal experience that the mind never fully stops moving.
This internal chaos explains why hyperfocus, the ability to lock into intense, sustained attention on specific things, does not contradict an ADHD diagnosis. The brain easily finds the chemical activation signal it needs from urgency, high interest, or novelty.
The real problem arises because most of what daily life requires doesn’t generate such a chemical signal.
The DSM-5 distinguishes true ADHD from situational inattention on this exact point: symptoms must be present across multiple contexts, not just when a task is genuinely boring. If a person zones out only in tedious environments, that is a normal human response, not a neurodevelopmental disorder.
ADHD without Hyperactivity Stays Hidden
Most people with inattentive ADHD develop intense compensatory strategies long before they ever get diagnosed.
These behaviors include obsessive list-making, multiple overlapping phone alarms, and showing up excessively early to buffer chronic time-management failures. In some cases, such tactics work well enough that the underlying condition isn’t as visible to others, even if the person experiencing it feels incredible amounts of overwhelm and shame.
High academic ability, often called being twice-exceptional or 2e, compounds the invisibility. High intellectual capacity allows some people to compensate well into adulthood, as good grades successfully hide the messy internal struggle.
Beyond intelligence, girls are especially likely to mask their symptoms because social expectations heavily reward quiet compliance.
The student who sits still and stares blankly at the wall does not get sent to the principal’s office. Instead, she is described as a daydreamer, placed in a slightly lower reading group, and told to apply herself.
This fragile masking usually breaks down during major life transitions, such as starting university, changing careers, or becoming a parent. When the external structure disappears, and the cognitive load becomes unsustainable, the system collapses.
That breakdown is typically when women wind up evaluated for anxiety or depression first, and ADHD much later, if at all.

Common Misconceptions About Inattentive ADHD
- Misconception 1: If you can focus on hobbies, you don’t have ADHD.
- The Reality: ADHD involves a dysregulation of attention, not its complete absence. Experiencing deep hyperfocus in high-interest or high-urgency situations is a hallmark symptom of the condition, meaning excellent performance in specific contexts does not rule out a diagnosis.
- Misconception 2: Adults eventually grow out of their ADHD.
- The Reality: While physical, hyperactive symptoms frequently decrease with age, internal inattentive symptoms usually persist throughout adulthood. A long-term clinical study by Biederman et al. on Adult ADHD Subtypes tracked diagnosed individuals and found that 93% of adults presented with either the inattentive or combined subtype, proving that the symptom profile shifts over time, but the real-world impairment does not.
- Misconception 3: Every individual who struggles to focus has inattentive ADHD.
- The Reality: Chronic inattention that tracks directly to untreated sleep deprivation, a major depressive episode, or acute anxiety should always be addressed first. A thorough medical evaluation explicitly rules out conditions that mimic inattentive symptoms before confirming an ADHD diagnosis.
Inattentive ADHD Quick Reference Guide
The table below compares the three primary ADHD presentations outlined in the DSM-5:
| Feature | Inattentive ADHD (ADHD-PI) | Hyperactive-Impulsive ADHD | Combined ADHD |
| Core Challenge | Sustaining attention, organizing, and task follow-through. | Impulse control and physical restlessness. | Both symptom clusters meet full diagnostic thresholds. |
| Visible to Others? | Often no. The struggle is largely internal and quiet. | Usually yes. The behavior is outwardly disruptive. | Yes. The challenges are both visible and internal. |
| Often Missed Until | Adulthood, and frequently missed entirely. | Childhood, usually spotted early in elementary school. | Childhood, though the inattention aspect may persist. |
| Gender Skew | Documented as more common in women. | Documented as more common in men. | Roughly equal distribution among adults. |
| Diagnosis Delay | Diagnosed an average of 5 years later than men. | Typically recognized and diagnosed much earlier. | Variable depending on coping mechanisms. |
| What It Looks Like | Daydreaming, losing tracking items, avoidance, and blanking mid-task. | Fidgeting, interrupting conversations, risk-taking, and impatience. | Exhibiting both daydreaming and physical fidgeting across settings. |
| Adult DSM-5 Threshold | 5 out of 9 designated inattention symptoms. | 5 out of 9 designated hyperactive symptoms. | 5 symptoms from each distinct cluster. |
Sources: Data compiled from clinical reviews via Psychiatric Times, the Journal of Attention Disorders, and Neurodivergent Insights.
What to Do Next
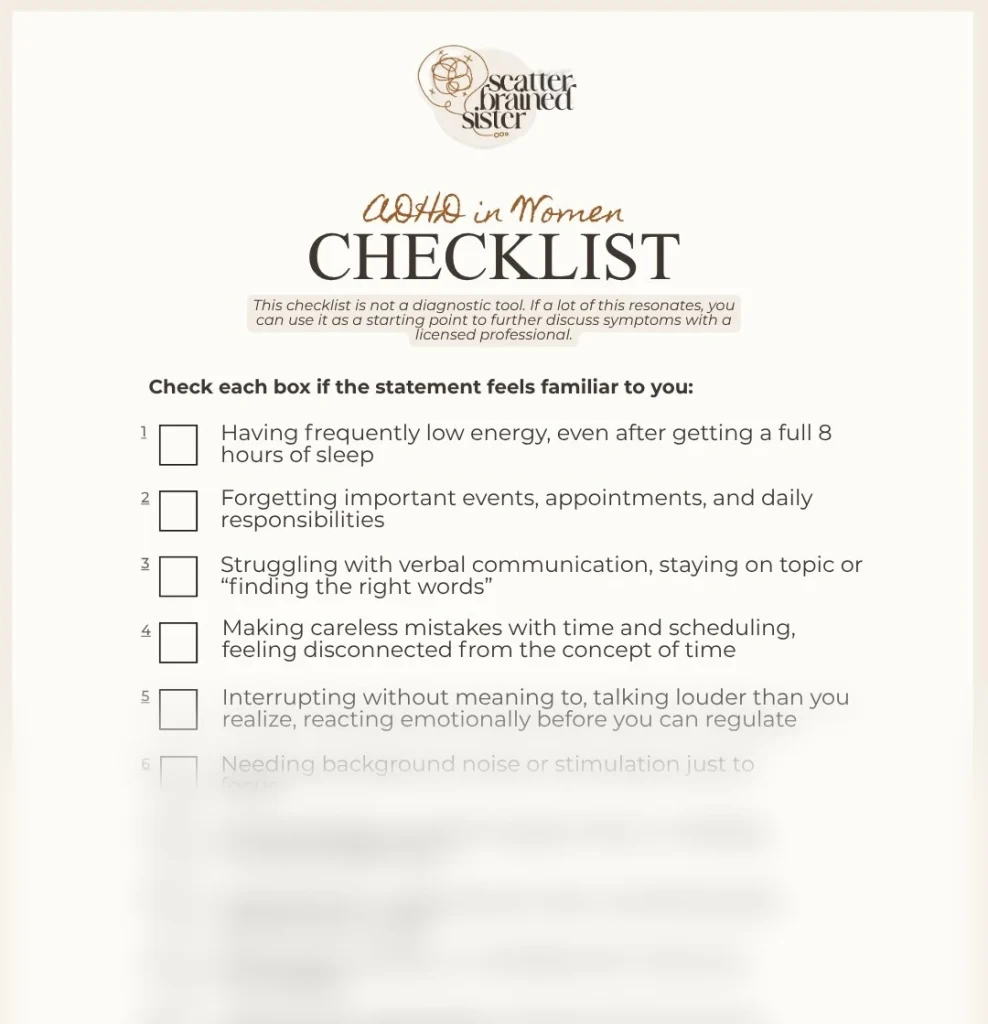
Step 1: Go Through an Adult ADHD Checklist
Go through the free ADHD in Women Checklist.
Clinical criteria read nothing like real life and are usually hard to see yourself in. Grab the ADHD in Women checklist, which translates formal medical criteria into what the condition truly looks like for an adult who has spent years feeling overwhelmed.
You can go through it and mark what you recognize for your own consideration or to bring to a doctor.
Step 2: Connect with Your General Practitioner or Therapist
Start your journey with whichever licensed professional you currently have access to. A general practitioner can begin the physical evaluation process directly and refer you to an expert psychiatrist.
While a standard therapist cannot issue a formal medical diagnosis, they can validate your experiences and provide the clinical referral needed to bridge the conversation with a doctor.
Go into the appointment prepared to describe exactly how these patterns impact your daily functioning.
Step 3: Complete an Evaluation
Your doctor will want to rule out alternative medical explanations first. Conditions such as thyroid imbalances, anemia, chronic sleep disorders, generalized anxiety, and clinical depression all produce cognitive patterns that overlap closely with inattentive ADHD.
A clinician needs to test for and account for these variables before confirming an ADHD diagnosis. Once these factors are evaluated, a targeted referral to a specialist ensures you receive the accurate support you need.
Frequently Asked Questions About ADHD Without Hyperactivity
Can a woman have ADHD without hyperactivity and go undiagnosed her whole life?
Yes, and population numbers strongly reflect this reality. Data compiled by CHADD on ADHD Gender Differences highlights that boys are historically diagnosed at roughly double the rate of girls.
Women presenting with inattentive ADHD frequently get treated for generalized anxiety or chronic fatigue first, which manages the secondary symptoms while the underlying neurological condition goes completely unexamined.
Is inattentive ADHD exactly the same thing as ADD?
Functionally, yes. ADD was the standard clinical label before the DSM-IV officially replaced the terminology in 1994. The correct medical term today is ADHD, predominantly inattentive presentation.
Some clinicians still use the acronym ADD informally to signal the total absence of physical hyperactivity, but the term carries no distinct diagnostic meaning on modern insurance documentation or school accommodation records.
Can you be diagnosed as an adult if you were never flagged as a child?
Yes. The DSM-5 requires that symptoms were actively present before the age of 12, not that a formal childhood diagnosis was actually recorded.
A thorough adult evaluation assesses your early childhood history through self-reporting, school report cards if available, and input from family members. The total absence of an early childhood diagnosis is itself frequently classic evidence of a missed inattentive presentation.
Summary
ADHD without hyperactivity is a recognized neurodevelopmental condition known as primarily inattentive ADHD.
It is defined by a chronic difficulty regulating your attention system, not by physical restlessness, and remains the most likely subtype to go completely undiagnosed.
The documented five-year diagnostic gap for women exists because inattentive symptoms are primarily internal. If these behavioral and cognitive patterns appear across multiple areas of your life and have impacted you for as long as you can remember, it is a step worth taking to schedule a formal conversation with a clinician.
Disclaimer: The content on Scatterbrained Sister is for informational and reflective purposes only and isn’t a substitute for professional medical advice, diagnosis, or treatment. Always consult your healthcare provider with questions about ADHD or any other condition. These experiences are personal and may not apply to everyone.